Question
This Assignment will be graded using this rubric: Week 11 Project Rubric (Word document). The “Week 11 Business Plan Excel Template” will guide the financial analysis portion of this assignment.
The Final Project Assignment:
Using the “Week 11 Project Business Plan Template”, create a business plan (8–10 pages) that includes the following:
Executive summary
Market analysis, including:
Macro- and microeconomic implications of market competition
ACO payment incentives to the organization
How the RUC impacts economic efficiency
Financial analysis, including:
Capital requirements
Reimbursement model
Cost per patient visit
Pro forma, including:
Patient revenue
Operating expense
Income from operations
Total expense
Net cash flow
Note: You must support your business plan with financial documents in an Excel spreadsheet. The 8- to 10-page paper requirement, submitted as a Word document, does not include the title, Excel spreadsheet, or reference pages. Your Assignment must be written in standard edited English. Be sure to support your work with specific citations from this module’s Learning Resources and additional scholarly sources as appropriate. Refer to the Essential Guide to APA Style for Walden Students to ensure that your in-text citations and reference list are correct. See the rubric for additional requirements related to research and scholarly writing.
Sample paper
Week 11 Project Business Plan Template
I. Executive Summary
The health of all the citizens in a country is paramount and not only to the urban people but also those who live in the rural areas. As a result, the government has encouraged the setting up of mobile clinics or rural urgent care facilities that are meant to attend the health needs of rural people. Urgent care comprises of the delivery of walk-in and is entirely focused on the delivery and provision of ambulatory care in a facility dedicated to the delivery of unscheduled, walk-in care outside of a hospital emergency department or room. Development of the Rural Urgent Care (RUC) facility in Sylacauga, Alabama will ensure that the common citizen has increased chances of accessing healthcare facilities than ever before. Mesa rural urgent care will facilitate access to care providers by extending the service hours that these healthcare providers are supposed to work (Heath, 2009). To achieve this objective, Mesa rural urgent care center needs to take their services within closer geographic proximity to patients, families, caregivers and healthcare stakeholders who can help to improve the health standard of the society in general. However, for the facility to operate effectively and efficiently, it needs to have a well-embedded director of the emergency who will head all the operation of the center. The appointed Director of Emergency Services will have the responsibility and duties to provide clinical monitoring to ensure quality service provisions and timely service delivery. The Mesa rural urgent care center will attempt to alleviate demand for emergency department (ED) services by moving lower critical patients to a less resource-intensive environment to ensure they receive the best care possible.
Vision
The facility’s vision is to bring the world-renowned and high-quality medical services close to the people of Nevada through the implantation and exploitation of high-level tools and machines and employment of skilled and knowledgeable individuals. We can achieve this through creating a professional business-client relationship. We will engage in sustainable duties while anticipating our clients’ needs and maximizing their satisfaction while maintaining quality services.
Mission
Our mission will be to provide each of our customers with best and quality services. We aim at improving their health to have a healthy population that can contribute to the economic development of the area. We work relentlessly to give customers the most compelling and quality services of all time. With time, we will move into contract clients to increase our customer base because Mesa rural urgent care center has the customers’ needs and desires at heart.
II. Program Overview: Market Opportunities and Utilization Patterns
Mesa rural urgent care center will attempt to provide treatment to patients suffering from non-life-threatening conditions that require quick attention, including bone fractures, pneumonia and flu, and minor lacerations and those suffering from life-threatening medical conditions will be taken to hospitals. Since the late 1980s and early 1990s, most of the high-profile hospitals have looked to facilities such as Rural Urban Centers to attend to serious issues before they can be taken to hospitals. These rural urgent centers are meant to reduce rates of inappropriate ED utilization by triaging non-emergent patients to less severe settings (Rust, 2009). The ED is not the most appropriate care setting for many patients, but they help in improving the condition of the patients before they can receive better and high-quality medical services. Non-urgent patients account for well over 10 percent of the average ED’s caseload and semi-urgent cases account for another 20 percent triaging non-emergent patients to less acute settings. However, just like any other hospital facility, the rural urgent care faces both market and nonmarket forces in the market. On the market forces of there is a hard reality that sustainable margins that are necessary for the financial viability of the care center. Additionally, the facility also faces nonmarket forces that are in the form of regulations employed by authorities to ensure they comply with the health standards of a country. The primary mission of any health care facility is caring for all people regardless of the economic power of the patients. At the other end of the critical spectrum, most emergent patients would be better served in an inpatient unit, but many are forced to board in the ED because beds are unavailable (Davidson, 2007).
To exercise fairness and justice to all, the facility will offer medical services in the order and degree of urgency, and the basis of first come first serve policy. Moreover, the center has a duty to recommend and transfer patients to an appropriate and well-equipped site where they can get proper care through the allocation of resources to meet patient acuity and results in better clinical outcomes. Rural Urban Center staffing and treatment approaches are fundamentally different from those in an ED; patients get more abbreviated and pointed clinical workups, which provides care more efficiently by clinicians who are oriented to less intense discovery and intervention. Additionally, due to the geographical location of the centers and increased number of service hours patients have higher chances of seeing the caregivers and doctors and have their medical issues addressed.
The Rural Urban Care center stands a good chance of providing competition to other hospitals considering that they are not subjects to the same regulations as permanent and high-level services. With the installation of new and highly efficiency equipment and tools and fewer overheads, rural urgent care facilities have an opportunity to capture higher margins and turn them to their advantages. However, if a problem needs a complex medical examination, the facility can always refer the patients to hospitals
The Rural Urban Care Center will address community needs for convenient, reliable access to care which is paramount to most of the citizens and the country in general. Current alternatives to Rural Urgent Care Centers s include the ED, which like other comparable United States and United Kingdom EDs, has long wait times and potentially stressful patient environments. Decreasing wait times is positively correlated with better outcomes considering that most of the patients only visit a medical center entirely based on the outcomes and results delivered by the health care providers of that particular facility. The facility will be a key factor in improving the length of stay and decreasing adverse events and mortality (Ruegg, 2013). On the same note, the Mesa rural urgent care center is a great pole to provide continuity of care and increasing adherence and compliance to the best practice guidelines as well as enhancing and improving communication among all the stakeholders and members of the healthcare team. In more than one occasion, urgent care centers have been found to match or surpass the care provided by hospitals making them popular among the low earners considering that they charge for many fees compared to big hospitals.
Services
The quality of the services offered by the Mesa rural urgent care center will be paramount and high quality in order to attract and maintain its current customer base. Customers, in this case, patient, are always sensitive and keen on the services that are provided by a healthcare facility and in that case provision of high-quality services is not an option. To meet the needs of the patients and the community at large in providing the appropriate level and necessary care without unnecessary duplication of a resource-intensive emergency department, the Rural Urgent Care center will seek to provide basic emergent procedures, diagnoses, and treatments (McDevitt, 2015). In extreme cases where the health condition of the patient is complex and hanging by the thread, the facility will provide care and services to sustain the patient’s life before getting him to a better and higher level hospital. Some of the services to be provided by the facility include:
• Nursing Triage – this involves the normal and formal medical process of accessing patients. Moreover, it comprises of accident and emergency services to ensure that victims receive the best and appropriate attention as possible.
• Physician assessments – physical assessments provided by the facility will include detailed documentation of all important information and details about a patient on the patient’s charts to make it easy for doctors to analyze their cases.
• Minor procedures – in situations and cases, where our healthcare providers need to perform minor procedures to save the patient’s life we will grandly perform the duties. The surgery performed in this facility must be involving little risk to the life of the patient.
• Basic lab services – the facility’s laboratory will be staffed with skilled laboratory technicians and personnel trained to provide high-quality results and accurate test results to provide timely assistance and help to the center’s physicians and doctors in diagnosing our clients’ health problems.
• Basic diagnostic imaging – the facility will attempt to employ visual representations of the interior parts of our client’s bodies for clinical analysis as well as medical intervention in the attempt to determine the extent of injuries and other internal body infections and problems.
• Vital signs – the basic service that will be provided by the facility is the measurement of the pulse rate, temperatures, blood pressure and respiration rate to give a clear status of the body functioning of all our patients.
• IV therapy – the facility will also offer intravenous therapy through the infusion of a liquid substance directly into the veins of our patients especially water or any other syrup. Moreover, the facility will also offer blood transfusion services.
• EKG – with the new and efficient machines the facility plans to install, it will be on a pole to test the electric activity of patients with heart problems through the use of electrocardiogram that shows the electric activity of the heart as line tracings in a paper.
• Wound care – wound care is one of the basic services that will be provided by the facility considering that wound from burns, and other injuries are common among people. The facility will offer services such as wound cleaning and dressing to ensure it is not affected and infected by bacteria.
Yearly Staffing Costs by Clinical Lead Model
The potential to house ambulance services out of the Rural Urgent Care Center provides additional requirements and opportunities in order to attend emergencies that may hit the surrounding community in an attempt to save their lives and helping them live happily. To accommodate the needs of the Emergency Medical Services crew that is an integral part of the facility, multiple waiting room/bunk rooms will be added to the facility. Moreover, creating a separate entry point for the ambulance service to save on time and avoid commotion and jam that may be witnessed in the main entry to the facility (Sabesan, 2012). Supplies will also be warehoused at the Rural Urban Center for easy restocking of ambulances and replenishment whenever the stock goes down. The Rural Urgent Care Center can also be part of the disaster-planning strategy by providing easy access to needed equipment and supplies during emergencies such as accidents, war, flood, and droughts.
Facility
Facility design must meet the needs of clinicians and consumers for the provision of a good and comfortable working environment. Consumers invariably associate the quality of healthcare services with the aesthetics of the site of care and as a result, having a clean, spacious and well-decorated facility is not an option but rather a necessity in ensuring that all customers are happy. The facility will be designed to blend into the local architecture to be a part of both the eastern and western communities since the facility management wants the community to feel like a part of the facility and the only way to honor their culture and practices is by incorporating their architecture designs. The Rural Urban Care facility will have the following basic space layout that will help the company to execute its plan and achieve the facility’s objectives and goals (DeVoe, 2009).
Facility Description
|
Space Description |
Quantity |
Square Feet Per Room |
Total Space |
|
| Central nursing/Physician station |
1 |
500 |
500 |
|
| Exam rooms |
5 |
100 |
500 |
|
| Treatment room |
1 |
150 |
150 |
|
| Radiology room |
1 |
200 |
200 |
|
| Staff offices |
2 |
100 |
200 |
|
| Reception/waiting area |
1 |
400 |
400 |
|
| Employee break room |
1 |
250 |
250 |
|
| Medical records |
1 |
250 |
250 |
|
| Laboratory |
1 |
200 |
200 |
|
| Restrooms |
3 |
50 |
150 |
|
| EMS facilities |
2 |
80 |
160 |
|
| Utility rooms |
2 |
150 |
300 |
|
| Subtotal: Usable Square Footage |
3,260 |
|||
| Circulation, mechanical, telecom/IT, other space |
915 |
|||
| Total Facility Size |
4,175 |
|||
Operating Model
For the facility to work effectively and efficiently, it has to put both the political and public opinion into considerations. However, sharing of hospital resources such as beds, operating rooms, and nurses is the priority of Mesa rural urgent care center. The political element of healthcare will help in decision-making processes that determine the success or failure of most operations in a hospital environment. The Rural Urban Care will open after the normal working hours of local physicians. These operating hours also align with the peak ED visit times, which significantly trail off after midnight. In addition, the facility will adopt an operating model framework that incorporates the need for patient classification techniques to be adopted and they form the basis of differentiating the techniques and methods to be applied to solve a health or medical problem (O’Cathain, 2008).
Our primary marketing will be online where we will use analytic-driven approaches. Social applications such as Twitter, Facebook, and Instagram will provide a good ground for commercialization. Our social pages will have photos that will promote consumer pride in our services. This policy will make it easy to get to more customers as most people are using the internet nowadays.
III. Market Profile
Market Overview
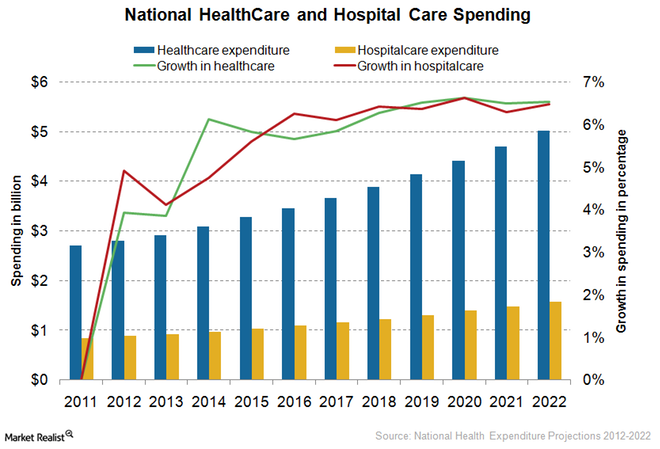
The United States healthcare sector comprises of different setups such as hospitals, walk-in clinics, emergency services and primary care providers. Some of these setups provide independent services while others vertically integrate to offer and provide a suite of medical services. As a result, the united healthcare sector is very competitive, and it requires efficiency and effectiveness as well as the provision of high-quality services to be in a position to compete for the ever growing market. With an increase in the aging population and the rise in the growth rate and birthrate, the healthcare market is expanding each and every single day. However, with the current rate of inventions and innovations, the sector is becoming competitive, and it requires constant review to ensure the facility will not be left behind (Poncelet, 2011).
Define your service area.
The facility is to operate and provide its services in Sylacauga, a city in Talladega County, Alabama a state in the United States. As at 2010, the city had more than 10,000 residents, and this is an ideal population to serve effectively using our facility. The total area of the city is estimated to be 50.9 km squared which is not hard to cover if the facility will manage high levels of efficiency and effectiveness
.
RUC Service Area
|
Area |
3 years ago |
2 years ago |
1 year ago |
||
|
Number of persons in RUC service area |
Total |
64,009 |
64,209 |
64,395 |
| Demand Forecasting |
Adjusted Demand of Services Forecast
Iv. Financial Analysis
Capital Requirements
Before the commencement of business, the facility needs to register the hospital with the authorities to obtain the license to carry on with their business. However, to have a business plan is crucial especially capital estimates. To estimate the total funds required for launch before the commencement of operations, the hospital has developed the following assessment of anticipated expenses related to the building of a single Rural Urban Care with 3,260 sq. ft. of usable space and 4,175 gross sq. ft., as described in an earlier section relating to facility design and a basic review of expected equipment costs.
Initial funding for the company will come from the original owners and investors of the facility. The owners decided to contribute three-quarters of the money while the rest of the findings will be obtained from the consolidated bank of New York. These funds were just enough to get into the enterprise basing on the high-quality machinery needed. It was agreed that the borrowed amount would be paid in installments for a period of one year (To, 2008).
Capital Requirements per RUC Site
| Total Construction Cost |
$3,246,605 |
| Contingencies, Professional Fees, Management & Overhead, Equipment |
$2,216,341 |
| Total Project Costs |
$5,462,946 |
Construction Costs per Square Foot $777.63
Project Costs per Square Foot $1,308.49
Square Footage 4,175
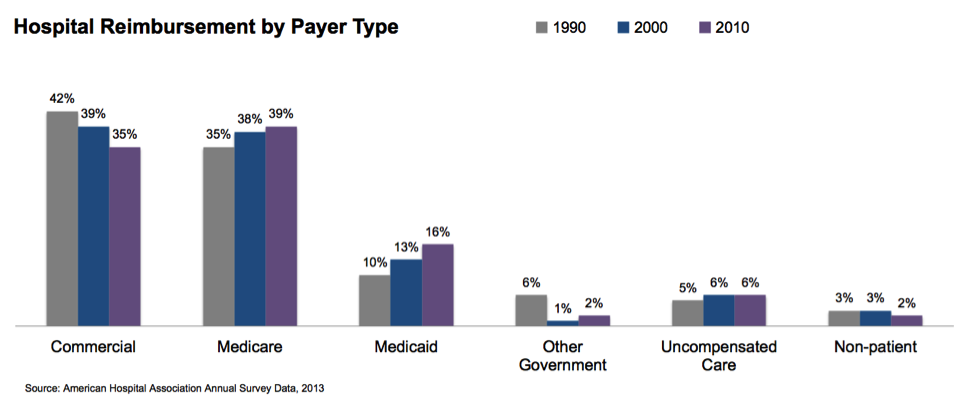
Reimbursement Model
The Rural Urban Care Center will charge a flat per-visit fee of $450, based on similar current hospital ED visit charges. This rate will stay constant. Contractual discounts for insurance is 30% of gross patient revenue. This will be the affordable rate for all levels of citizens ranging from high earners to low earners who may have the privilege of visiting the facility (McDevitt, 2015).
Services Offered
| Nursing Triage
Physician Assessments |
Potential Diagnoses Common illness Respiratory illness Allergies Bladder infections Eye/ear/sinus infection Strep throat Mononucleosis Pregnancy testing Skin rashes Sport injuries/sprains/strains |
| General Services | Monitoring Services
Emergency transfer to KEMH Vital signs IV therapy (antibiotic, hydration) EKG Wound care Immunizations, TD, Pneumovax, Flu Vaccines |
|
Minor Procedures Incision and draining of abscess Excision of skin Aspiration of cyst Sutures |
|
|
Lab Services Blood Urine Other |
|
|
Diagnostic Imaging Ultrasound X-ray |
Reference
Davidson, M. B. (2007). Effect of a nurse-directed diabetes disease management program on urgent care/emergency room visits and hospitalizations in a minority population. Diabetes Care, 30(2),, 224-227.
DeVoe, J. E. (2009). Do children in rural areas still have different access to health care? Results from a statewide survey of Oregon’s food stamp population. . The Journal of Rural Health, 25(1),, 1-7.
Heath, B. S. (2009). Pediatric critical care telemedicine in rural underserved emergency departments. . Pediatric Critical Care Medicine, 10(5), , 588-591.
McDevitt, J. &. (2015). An evaluation of the quality of Emergency Nurse Practitioner services for patients presenting with minor injuries to one rural urgent care centre in the UK: a descriptive study. . ournal of clinical nursing, 24(3-4), 523-535.
O’Cathain, A. C. (2008). Characteristics of the emergency and urgent care system important to patients: a qualitative study. . Journal of Health Services Research & Policy, 13(suppl 2), , 19-25.
Poncelet, A. B. (2011). Development of a longitudinal integrated clerkship at an academic medical center. Medical education online,, 16.
Ruegg, T. A. (2013). A nurse practitioner-led urgent care center: meeting the needs of the patient with cancer. . Clinical journal of oncology nursing, 17(4), , E52.
Rust, G. B. (2009). Presence of a community health center and uninsured emergency department visit rates in rural counties. . The Journal of Rural Health, 25(1), , 8-16.
Sabesan, S. L. (2012). Telemedicine for rural cancer care in North Queensland: bringing cancer care home. Australian journal of rural health, 20(5),, 259-264.
To, T. C. (2008). Can a community evidence-based asthma care program improve clinical outcomes?: a longitudinal study. Medical care, 46(12), , 1257-1266.